Synergies with other Cannabinoids, Mechanisms of Action, and Benefits Supported by Clinical Data
This is a comprehensive review of existing scientific work and clinical studies on Cannabinol (CBN) and its mechanisms of action inside the human body. Clinical evidence of dose dependent synergistic effect of taking CBN with other cannabinoids is discussed, along with revealing the truths and myths of its benefits. As with most cannabinoids, the accurate human clinical and scientific evidence of CBN benefits is very hard to find, so this review focuses on the existing clinical trials, analyzes the results and summarizes the findings into one comprehensive report. Findings suggest that CBN may be beneficial as a relaxation and sleep aid, pain relief support, anti-bacterial agent and help against various dermatologic and bone disorders. Evidence of synergistic effects of using CBN coupled with other cannabinoids also exists. But first, lets discuss what CBN is, and how it interacts with the human endocannabinoid system.
Cannabinol (CBN) and Cannabinoid Receptors (CB1 and CB2)
As a result of synthase reactions between the Mother Cannabinoid (CBGA) and various enzymes that exist in the particular strain of hemp in the environment that provides the necessary thermal, photolytic and oxidative conditions, major Phyto-cannabinoids (CBDA, Δ9-THCA, and CBCA) are synthesized. However over time, due to heat, light and oxidation Δ9-THCA degrades into Cannabinolic Acid (CBNA).
After the hemp plants (<0.3% of total Δ9-THC) are harvested and decarboxylated, Cannabinolic Acid (CBNA) turn into its base form Cannabinol (CBN), which is considered more active and potent than its acid form (Figure 1). In order to understand how CBN works in the human body we will first review the cells and receptors it interacts with in the human endocannabinoid system.
Figure 1. Chemical structures of A: Cannabinol (CBN) and B: Cannabinolic Acid (CBNA)
The biological effects of cannabinoids are mediated by Cannabinoid Receptors CB1 and CB2(1). CB1 receptors are present in the membranes of the Central Nervous System (CNS) cells that are located throughout the body, but mostly concentrated in the brain (2). CB2 receptors are present in the membranes of the immune system cells and even though those cells can also be found throughout the body, they are mostly concentrated in the GI Tract(2). Research has shown that activation of CB1 and CB2 receptors results in the biological responses in the brain, liver, reproductive system, immune system, cardiovascular system, musculoskeletal system, heart and the GI tract (See Figure 2(3)).
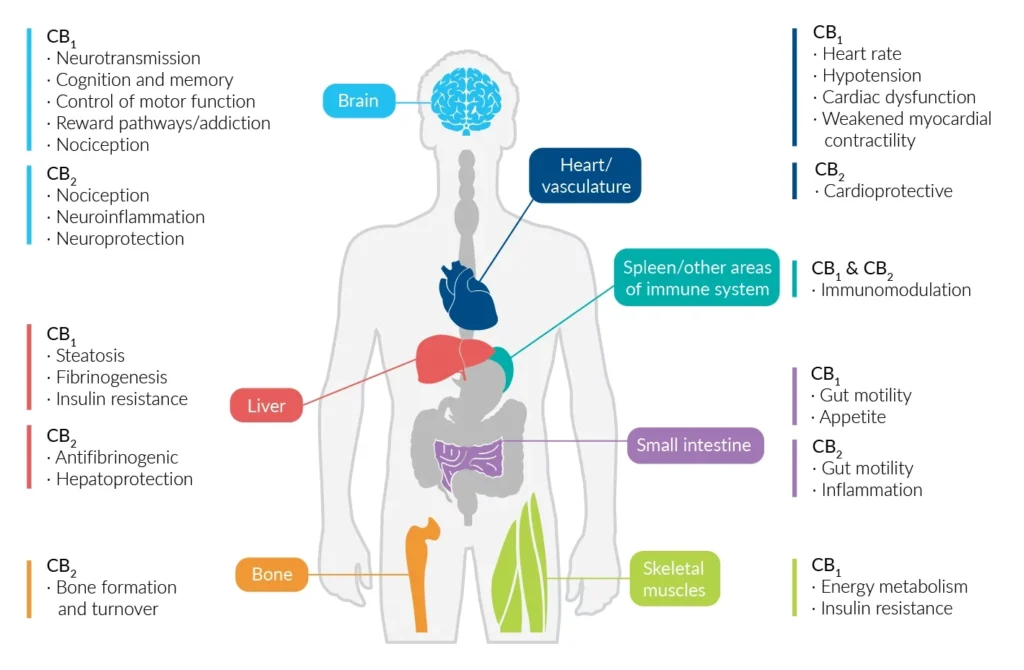
Figure 2. Major localization sites and associated functions of the CB1 and CB2 receptors in the human body. (Picture taken from (3))
CBN in Combination with CBD as a Pain Relief Support
A 2019 clinical study performed by Hayes Wong and Brian E. Cairns investigated whether non-psychoactive cannabinoids, Cannabidiol (CBD), Cannabinol (CBN) and their combinations can increase pain tolerance. The study has shown that a (1:1) blend of CBN and CBD provided longer-lasting pain relief than CBN alone, or CBD alone, showing that when it comes to pain management, CBN may be a great complement to CBD, and while CBN alone is a viable pain relief option, a combination of CBN and CBD is even better (4). Figure 3 shows the influence of CBD and CBN on the pain tolerance compared to the Vehicle, which is the Control.
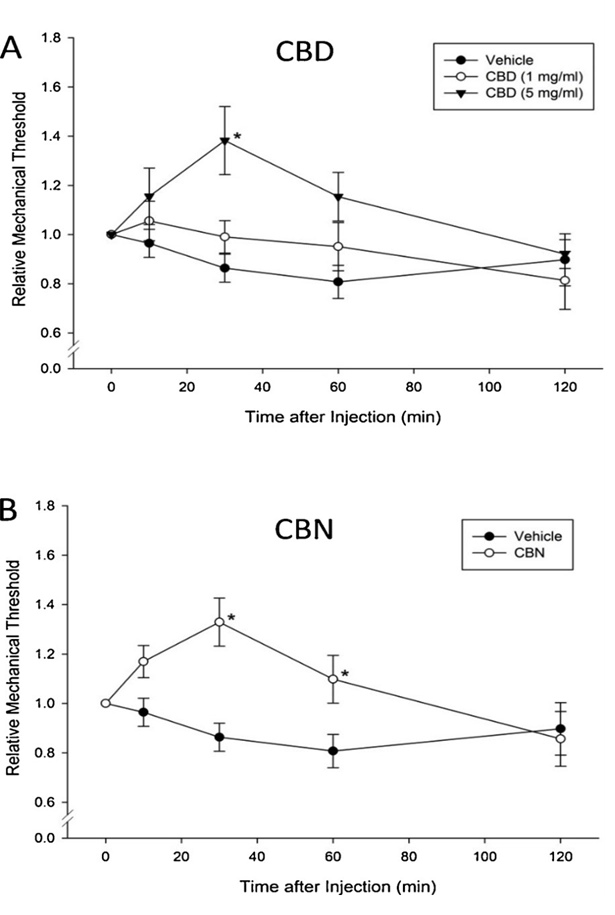
Figure 3. (A) (4) shows how the relative pain threshold changes over 2 hours, after CBD at 1mg/ml and 5mg/ml as well as the vehicle by itself are administered. The study clearly shows that the pain tolerance sharply increases in a dose dependent manner. (B) (4) shows a similar pain threshold changes over 2 hours, after CBN at 1mg/ml compared to the vehicle by itself.
However, various combinations of CBD and CBN (at the ratios of 1:1 and 5:1) show vastly different results (see Figure 4).
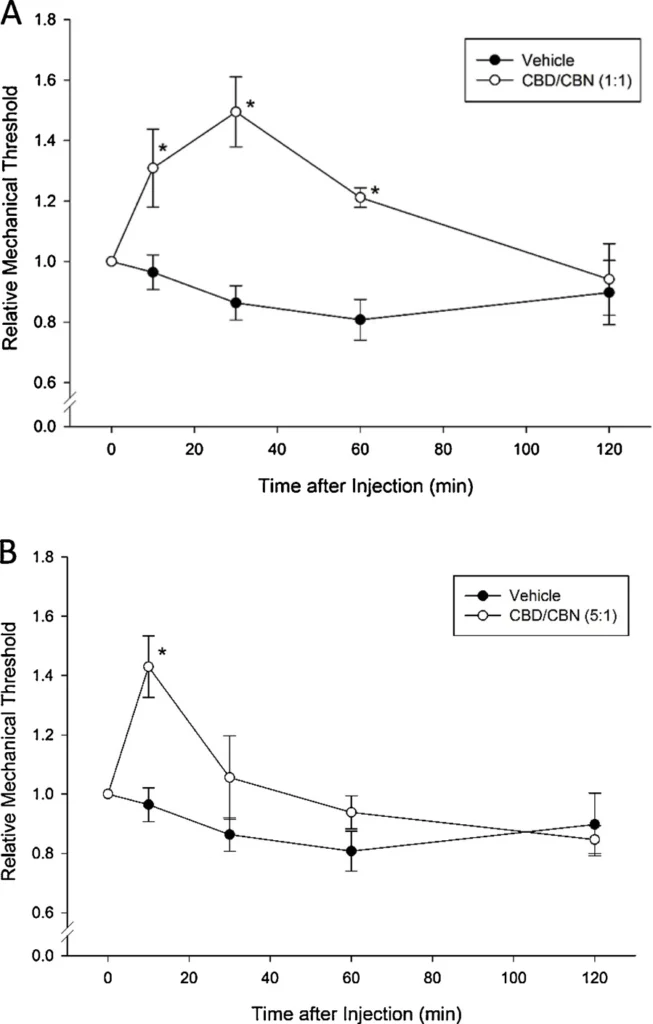
Figure 4. (A) (4) shows that combination of CBD:CBN (1:1) shows a superior relative pain tolerance of about 1.5 within about 30 minutes, followed by a decrease to about 1.0 within the next 90 minutes, showing that the equal combination of CBD and CBN results in the best relative pain tolerance for the longest duration compared to CBD , CBN and the vehicle individually. (B) (4)shows that a (5:1) combination of CBD to CBN reduces the intensity and duration of the pain relief in comparison to the (1:1) combination of CBD to CBN, which may indicate an inhibitory effect of higher concentration of CBD on CBN (4).
These results are not surprising since after administration CBN interacts directly with CB1 and CB2 receptors in the immune and nervous systems of the Endocannabinoid System, whereas CBD interacts with the TRP channels in the cell membranes. Figure 2 demonstrates that any cannabinoid that bonds to CB1, or CB2 receptors causes anti-nociceptive effects, or analgesia. For example: Δ9-THC is by far the strongest analgesia inducing cannabinoid known simply because its affinity to CB1 receptors is the strongest. CBN on the other hand, has a strong affinity towards CB2 receptors, and a weaker affinity towards CB1 receptors, which means that the physiological response to CBN includes analgesia and anti-inflammation among many other responses. It is also well known that CBD activates and desensitizes TRPA1 channels which are responsible for pain signal propagation. So the study results make sense, because a combination of activating CB1 and CB2 receptors along with desensitization of TRPA1 channels, which modulate pain signals, in a balanced way (1:1 CBD:CBN) should result in pain relieve. However, the non-psychoactive cannabinoids CBD and CBN were less efficacious than Δ9-THC at the same concentration (1 mg/ml) in reducing pain and sensitization(4). This is not surprising, as these cannabinoids have weaker binding affinity for the CB1 receptors when compared to THC: CBN (˜1/10th), CBC (˜1/20th) and CBD (˜1/100th)(5). However CBD and CBN are non-psychoactive, hence using them for pain relief is more advantageous than Δ9-THC, because psychoactive effect of Δ9-THC is an important limitation of THC use for analgesia(6, 7, 8).
Effect of CBN on Bone Growth and Collagen Production
Recently, the cannabinoid receptors CB1 and CB2 were shown to modulate bone formation and resorption in vivo, although little is known of the mechanisms underlying this (9). The clinical study reviewed below found that cannabinoids, especially CBN, may stimulate the recruitment of Stem Cells (SC) from the bone marrow mediated via the CB2 receptor, which may be the mechanism responsible for the increased bone formation seen after cannabinoid treatment in vivo. CB2 receptors have been found in normal skin and now in bone tissue (10, 11), where they are thought to play a role in regulating bone mass in humans (12), and CB1 receptors play a role in the regulation of bone mass mediating bone resorption, thus preserving bone mineral density(11).
It is widely accepted that the stem cells from bone marrow play a central role in bone physiology and pathology, and they can transform into other cell types including cardiomyocytes(13), muscle cells(14), and neural cells(15). The physiological function of Bone Marrow Stem Cells is still unclear; however, it is possible that they are involved in tissue healing processes such as muscle regeneration(16) and fracture healing(17).
In 2007 (Scutt and Williamson) treated the Bone Marrow Stem Cell Fibroblastic Colony-Forming Unit (CFU-f) cultures with a variety of naturally occurring cannabinoids, including Cannabidivarine (CBDV), Cannabigerol (CBG), Cannabinol (CBN), Cannabidiol (CBD), THC, and Tetrahydrocannabivarin (THCV), and all at 10 µM, produced a stimulation of colony formation in all cases, which was accompanied by collagen synthesis as well (see Figure 5)(9).
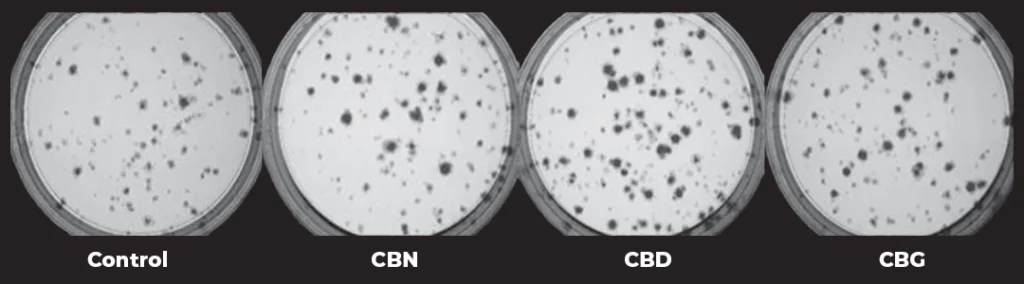
Figure 5(9). The effect of CBN, CBD and CBG cannabinoids on connective tissue colony formation by Bone Marrow Stem Cells in-vitro compared to the Control.
Also observed were increases in Collagen and Alkaline Phosphatase (APase) (see Figure 6)(9), which is a marker for B cell activation(18), which is a key player of the adaptive immune response in mammals(19). B-cell production in humans is a lifelong process that starts in the fetal bone marrow after birth(19).
The study by (Scutt and Williamson) demonstrated that cannabinoids like CBN, CBD and CBG can stimulate the formation of Stem Cells inside the Bone Marrow, which play a central role in a wide range of physiological and pathophysiological processes, including bone formation, fracture healing, muscle regeneration, vascular damage, atherosclerosis, bone marrow fibrosis, as well as support of hematopoietic stem cells(9). In addition, many therapeutic applications for the Bone Marrow Stem Cells have been suggested, including among many others myocardial regeneration; tissue engineering of bone, cartilage, and vascular tissue; and cell or gene therapy of genetic conditions such as osteogenesis imperfecta and muscular dystrophy(9).
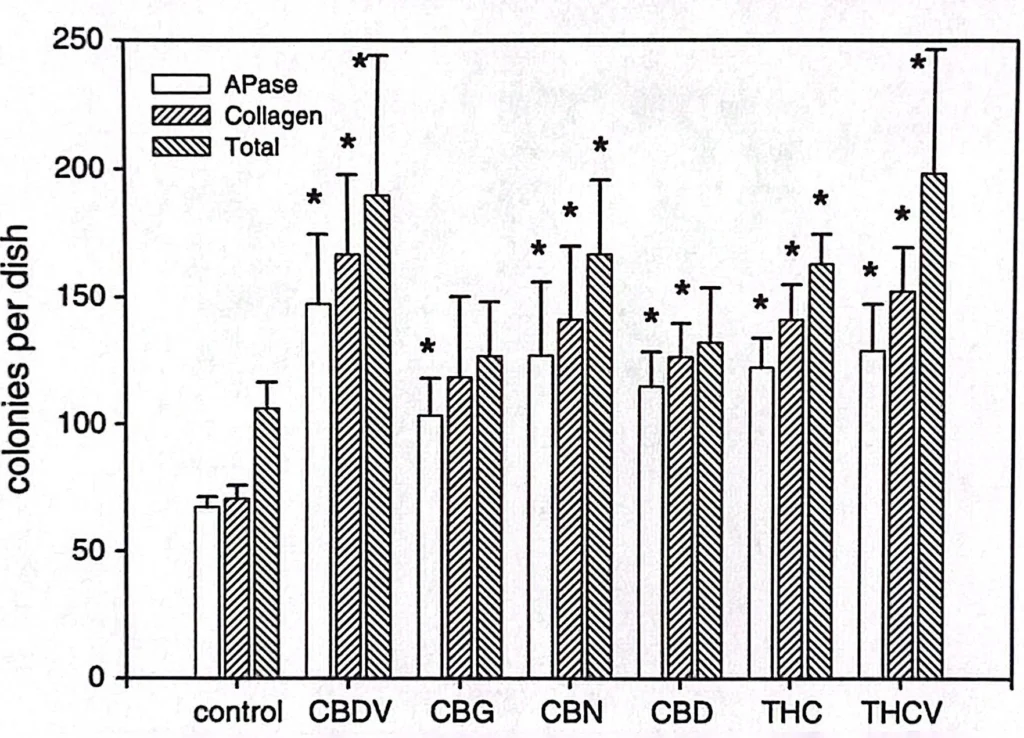
Figure 6(9). The effect of various cannabinoids on connective tissue colony formation by Bone Marrow Stem Cells in-vitro. In particular the formation of Alkaline Phosphatase (APase) enzymes due to the plasma immune system activation and Collagen.
This means that there is a potential for a significant synergistic effect of all these benefits if Cannabinoids like CBN, CBD, CBG and others are combined.
CBN as a Powerful Anti-Bacterial Agent
Recent studies suggest that CBN may have powerful antibacterial properties. It has been proven to be more powerful against dental bacteria that causes cavities, bad breath, and tooth decay, than Oral B, Colgate and other oral care products. These bacteria accumulate in the dental plaque, which is a complex biofilm that gets formed on the teeth and acts as a reservoir of different microbes. It is the root cause for the occurrence of several dental problems and diseases, including cavities, bad breath, bleeding gums, tooth decay, and tooth loss. Therefore, it should be regularly removed using suitable oral care aids(20).
A first of its kind study performed by (Stahl et. al.) in 2020 compared the efficacy of the best oral care products on the market and cannabinoids in reducing the bacterial content of dental plaques(20).
Dental plaque refers to the complex biofilm that acts as a reservoir of several microbes that can be defined as “the soft deposit that forms the biofilm adhering to the tooth surface or other hard surfaces in the oral cavity, including removable and fixed restorations”(21). Dental plaque is formed owing to the deposition of a combination of saliva, foods, and fluids on the tooth surface(21). The dental plaque formed on the tooth surface and gum line includes thousands of bacteria that convert food residues into acids, eventually leading to the initiation of dental diseases such as dental caries, gingivitis, and periodontal diseases(21). Periodontitis or gum disease is a global public health problem that affects millions of people each year and is the most common cause of tooth loss in adults(21). It is a gum infection that affects the soft and hard tissues supporting the teeth (see Figure 7)(22).
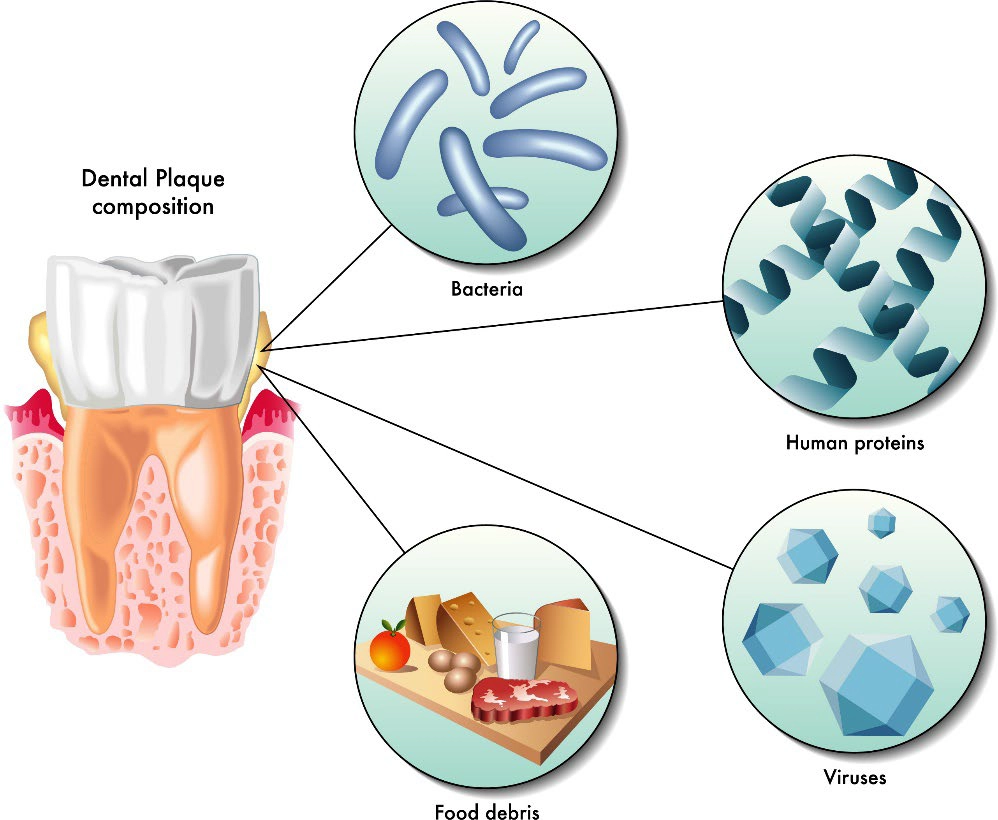
Figure 7. Representation of a dental plaque as the primary cause of gingivitis.
In the unique study by (Stahl et. al.) 60 adults aged 18 to 45 years were categorized into six groups based on the Dutch periodontal screening index. Dental plaques of the adults were collected using paro-toothpick sticks and spread on two Petri dishes, each with four divisions. On Petri dish-A, Cannabidiol(CBD), Cannabichromene (CBC), Cannabinol(CBN), and Cannabigerol(CBG) were used, and on Petri dish-B, Cannabigerolic Acid(CBGA), Oral B, Colgate, and Cannabite F (a toothpaste formulation of pomegranate and algae) were used. The Petri dishes were sealed and incubated, followed by counting the number of colonies(20). By evaluating the colony count of the dental bacteria isolated from six groups, it was found that cannabinoids were more effective in reducing the bacterial colony count in dental plaques as compared to the well-established synthetic oral care products such as Oral B and Colgate proving that Cannabinoids have the potential to be used as an effective antibacterial agent against dental plaque-associated bacteria and provides a safer alternative for synthetic antibiotics (like the golden standard Chlorhexidine Digluconate, Colgate and Oral B) to reduce the development of drug resistance (20).
The participants in the study were categorized into six groups (10 participants in each group) on the basis of Dutch periodontal screening index (DPSI) as follows: 0, perfect gum and no bleeding; 1, inflammation and bleeding of gum (gingivitis); 2, conditions of category 1 and chalk hardened dental plaque; (-3), conditions of category 2 with bone involvement (periodontitis); (+3) conditions of (-3) with recessions of gum and root exposure; and 4, conditions of category (+3) with severe bone resorption and high tooth mobility(20). See Figure 8 for results.
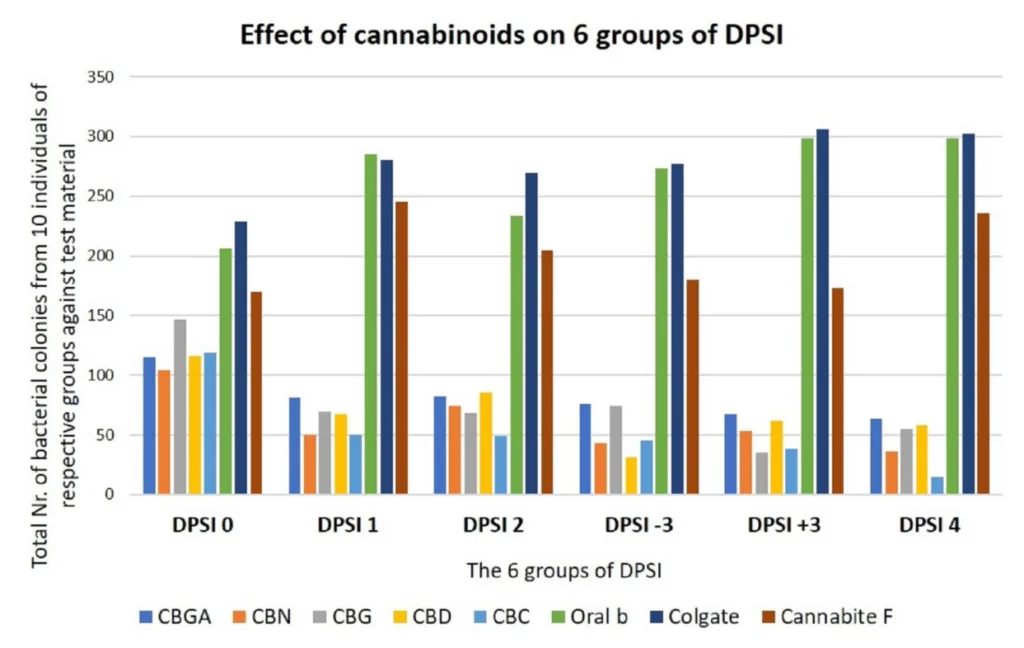
Figure 8. Comparison of six research groups with respect to bacterial colony count.
As can be seen from Figure 8 the results showed that cannabinoids were found to be more effective in reducing the colony count of the bacterial strains (gram-positive bacteria, such as Streptococcus mutans, followed by gram-negative bacteria and several other anaerobes such as Fusobacterium and Actinobacteria) as compared to the well-established synthetic oral care products such as Oral B or Colgate(20). As can also be seen, there may be a significant synergistic effect if Cannabinoids like CBN, CBD, CBC, CBG are combined.
It was also suggested that CBN, CBD, CBC, and CBG cannabinoids showed activity against a variety of Methicillin-Resistant Staphylococcus Aureus (MRSA) strains of current clinical relevance like (, however the mechanism of this powerful anti-bacterial activity is very elusive(23).
Table 1 shows the activity of CBD, CBC, CBG, and CBN against Staphylococcus Aureus strains that includes the infamous EMRSA-15 and EMRSA-16, SA-1199B a multidrug-resistant strain, a macrolide-resistant strain (RN4220), a tetaracycline-resistant strain (XU212), and a standard laboratory strain (ATCC25923). The activities were compared highly favorably with the standard antibiotics for these strains (Norfloxathin, Erythromycin, Tetracyclin, and Oxacillin)(23).
| Compound | SA-1199B | RN-4220 | XU212 | ATCC25923 | EMRSA-15 | EMRSA-16 |
| CBD | 1 | 1 | 1 | 0.5 | 1 | 1 |
| CBC | 2 | 2 | 1 | 2 | 2 | 2 |
| CBG | 1 | 1 | 1 | 1 | 2 | 1 |
| CBN | 1 | 1 | 1 | 1 | 1 | 1 |
| Norfloxathin | 32 | 1 | 4 | 1 | 0.5 | 128 |
| Erythromycin | 0.25 | 64 | >128 | 0.25 | >128 | >128 |
| Tetracyclin | 0.25 | 0.25 | 128 | 0.25 | 0.125 | 0.125 |
| Oxacillin | 0.25 | 0.25 | 128 | 0.125 | 32 | >128 |
These in-vitro studies showed that on average at 1µg/mL CBN, CBD, CBG and CBC are very effective against MRSA strains and for many strains are much more effective than the conventional anti-biotic medication currently used in the world. Moreover, a combination of these cannabinoids (especially CBN and CBD) would be even more effective due to the synergistic effect they would provide.
Studies and Research on CBN as a Sleep Aid
Currently, CBN is almost exclusively marketed as a sleep aid, but is there really scientific basis for this, or is it a myth? This question arises because it is very hard to find any credible clinical studies or research evidence that CBN helps with sleep.
The first study on the effects of CBN on humans was performed in 1975, when Δ9-THC and CBN were administered to 5 male volunteers with 1 week of rest in between doses. The doses were as follows: “placebo, 50 mg CBN, 25 mg Δ9-THC, 12.5 mg Δ9-THC + 25 mg CBN, and 25 mg Δ9-THC + 50 mg CBN (orally)(24). The study showed that CBN alone produced no change in physiological conditions(heart rate, electrocardiogram, blood pressure, or body temperature), and no change in psychological conditions(feeling of being drugged, drunk, dizzy, and drowsy). Δ9-THC by itself produced an increase in heart rate and change in psychological condition(feeling of being drugged, drunk, dizzy, and drowsy). With combined CBN+ Δ9-THC treatment, volunteers reported feeling more drugged, drunk, dizzy, and drowsy than under the Δ9-THC condition alone. None of the drug treatments produced significant changes on perception, emotion, cognition and sociability(24). So it may appear that CBN increased the effect of Δ9-THC on some aspects of physiological and psychological processes, but these effects are small and cannot account for the greater potency which has been reported when plant material is used(24).
In another study also performed in 1975(25), oral doses of Δ9-THC 20 mg, combined with placebo or with 40 mg doses of Cannabinol (CBN) and Cannabidiol (CBD), were given to volunteers. The combination of THC with CBN produced no detectable changes in the quality, intensity, or duration of the effects of THC alone. The THC-CBD combination tended to delay onset and prolong effects of THC, while making them somewhat more intense(25). Even this interactive effect was slight, providing no reason to conclude that CBN, or CBD have any effect on sleep separately, or when combined with THC.
So here we have 2 studies that directly contradicted each other. In recent years, marketers of hemp and cannabis products have claimed that Cannabinol (CBN) has unique sleep-promoting effects(26), but the early pre-clinical and clinical research investigating the effects of CBN is dated and limited, with most of human studies occurring in the 1970-1980s with small sample sizes lacking diversity in sociodemographic characteristics(26). Randomized, double-blind, placebo-controlled studies specifically assessing subjective effects associated with sleep, such as sedation or fatigue, were non-existent until August of 2023 when (Isobel Lavender et.al.) published their protocol for randomized, double-blind, placebo-controlled, cross-over, three-arm, proof-of-concept trial, which is currently in process investigating the effects of CBN on sleep and next-day function in 20 participants with clinician-diagnosed insomnia disorder and an Insomnia Severity Index Score ≥ 15. Participants receive a single fixed oral liquid dose of 30 mg CBN, 300 mg CBN and matched placebo, in random order on three treatment nights; each separated by a 2-week wash-out period. Participants undergo overnight sleep assessment using in-laboratory polysomnography and next-day neurobehavioral function tests(27). The primary outcome is wake after sleep onset minutes, secondary outcomes include changes to traditional sleep staging, sleep-onset latency and absolute spectral power during non-rapid eye movement (NREM) sleep, tertiary outcomes include changes to sleep spindles during NREM sleep, arousal indices, absolute spectral power during REM sleep and subjective sleep quality, safety-related and exploratory outcomes include changes to next-day simulated driving performance, subjective mood and drug effects, postural sway, alertness and reaction time, overnight memory consolidation, pre and post-sleep subjective and objective sleepiness; and plasma, urinary, and salivary cannabinoid concentrations(27). This first of its kind study will provide novel preliminary data on CBN efficacy and safety in insomnia disorder, which will inform larger clinical trials.
There is a plausible mechanism of action, because CBN does interact with CB1 receptors. The interaction is weak, so the “sleep” effect may be highly dose dependent, which means dosages significantly higher than those found in currently available CBN products marketed for sleep (typically ≤5 mg) are needed, but in order to know the right dose of CBN that would induce sleep, we need to know how much less psychoactive CBN is than Δ9-THC.
Evidence of psychoactive effect in humans suggests reduced potency relative to Δ9-THC and very poor oral bioavailability of CBN. For example, Hollister (1973) administered oral CBN (20–400 mg) to males without any “characteristic mental or physical effects of THC”, similarly, Karniol et al. (1975) reported no THC-like effects with oral CBN (50 mg) in males, however, CBN (IV, 194 μg/kg) produced Cannabis-like effects that were reported to be mild and enjoyable in males with substantially (~10-fold less) less potency than Δ9-THC (Perez-Reyes et al., 1973)(28). However (Ethan Russo et al., 2017) found that relative to THC, CBN maintains about ¼ the potency(29), but sadly only measurable after intravenous administration(30).
Based on the currently available clinical and research studies on CBN and sleep, we can conclude that the bioavailability of CBN isolate/oil is very low and to have a positive effect on sleep without ingesting grams of CBN isolate, its bioavailability will need to increase significantly. The best way to achieve that is through creation of stable oil-in-water liquid emulsion of CBN in water through nano-emulsification “Water Soluble CBN”.
Best Water-Soluble Cannabinoid Maker on the Market
Mile High Labs develops the best Water Soluble Cannabinoids on the market, which includes water soluble powders and liquids of CBD, CBG, CBN and soon CBC isolates and distillates. Here are the advantages of using MHL water soluble liquids:
- MHL Water Soluble Cannabinoids (powders and liquids) contain 20% active loading of Cannabinoids(CBD, CBG, CBN). Which means every mL of MHL liquid emulsion contains 200mg of the specific Cannabinoid v.s. the competition that only contains at most 5%-10% loading. This means that one would have to add 2-4 times less of MHL water soluble liquid than the competition and consequently the price of this ingredient would be greatly reduced if MHL products are used.
- MHL Water Soluble Cannabinoids have 24 month physical, microbiological, and chemical stability, which means the emulsion does not separate and the Cannabinoids don’t degrade if kept at room temperature for 24 months. The competition can only claim at most 12 months stability.
- MHL Water Soluble Cannabinoids only use natural ingredients including emulsifiers. Competitive products on the market use synthetic Polysorbates and other polymers that could be harmful if used at large amounts.
- MHL Water Soluble Cannabinoid emulsions are made up of micelles with the d(50) diameter of 250nm with the particle size distribution from >100nm to 350nm. So they are allowed to be used as ingredients in UK and EU because the smallest micelles have a diameter of >100nm, but the largest micelles have sizes not so large that it introduces instability and low bioavailability. The micelle size distribution is carefully optimized to maximize Cannabinoid bioavailability and minimize their bitter taste, while keeping the emulsion stable for 24 months at room temperature.
Competitive products on the market either are nano-emulsions with droplet sizes of <100nm, which are not allowed to be sold and used in UK and EU, or have droplet sizes upwards of 500nm-600nm, which impacts the bioavailability of the Cannabinoids.
Conclusion
This comprehensive review of the currently proven and disproven CBN benefits discusses hoe CBN interacts with the human endocannabinoid system (CB1 and CB2 receptors), the existing evidence of CBN and CBD combination as an effective help for pain relief, evidence of CBN helping with osteoporosis due to it’s activity in bone growing and collagen production, evidence of CBN as a very effective anti-bacterial agent including infamous strains of MRSA and bacterial in the dental plaque, as well as a discussion on CBN as a sleep aid, which is currently very controversial in that currently it is globally marketed and accepted as a sleep aid, but due to its very low bioavailability and very low activity the current data only supports it as a sleep aid after IV injection and not oral intake. Furthermore, a claim that currently the most marketed dose of 5mg is effective as a sleep aid is unsubstantiated . To increase the bioavailability of CBN to the point where it is effective at low doses, one must consider the Water Soluble Liquid of CBN. This oil-in-water emulsion based delivery system would deliver considerably more CBN into the blood circulation and all the above benefits of CBN reviewed may be amplified.
References
- Shenglong Zou and Ujendra Kumar “Cannabinoid Receptors and the Endocannabinoid System: Signaling and Function in the Central Nervous System” International Journal of Molecular Science, 2018 Mar; 19(3): 833
- Bihua Bie, Jiang Wu, Joseph F. Foss, and Mohamed Naguib “An overview of the cannabinoid type 2 (CB2) receptor system and its therapeutic potential”. Current Opinions in Anesthesiology 2018 Aug; 31(4): 407–414
- “Cannabinoid Signaling: Insights to Future Pharmacotherapeutic Development” Cayman Chemical Article from 2020-09-03
- Hayes Wong, Brian E. Cairns “Cannabidiol, cannabinol and their combinations act as peripheral analgesics in a rat model of myofascial pain”. Archives of Oral Biology, 104 (2019) 33-39
- Pertwee, R. G. (2008) The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: delta9-tetrahydrocannabinol, cannabidiol and delta9-tetrahydrocannabivarin. British Journal of Pharmacology, 153, 199–215
- Amar, B. (2006). “Cannabinoids in medicine: A review of their therapeutic potential”. Journal of Ethnopharmacology, 105, 1–25
- Izzo, A. A., Borrelli, F., Capasso, R., Di Marzo, V., & Mechoulam, R. (2009). “Non-psychotropic plant cannabinoids: New therapeutic opportunities from an ancient herb”. Trends in Pharmacological Sciences, 30, 515–527
- Pertwee, R. G. (2005). “Pharmacological actions of cannabinoids”. Handbook of Experimental Pharmacology, 1–51
- A. Scutt, E. M. Williamson “Cannabinoids Stimulate Fibroblastic Colony Formation by Bone Marrow Cells Indirectly via CB2 Receptors” Calcified Tissue International (2007) 80:5059
- Bab I, Ofek O, Karsak M, Fogel M, Wright K, AttarNamdar M, Shohami E, Zimmer K, Mechoulam R (2004) “Cannabinoid CB2 receptor and human osteoporosis”. 14th Annual Symposium, International Cannabinoid Research Society, Paestum, Italy, p P74, 22-24 June 2004
- Idris AI, van ’t Hof RJ, Greig IR, Ridge SA, Baker D, Ross RA, Ralston SH (2005) “Regulation of bone mass, bone loss and osteoclast activity by cannabinoid receptors”. Nat Med 11:774-779
- Karsak M, Cohen-Solal M, Freudenberg J, Ostertag A, Morieux C, Kornak U, Essig J, et al. “Cannabinoid receptor type 2 gene is associated with human osteoporosis. Hum Mol Genet 14:3389-3396
- Toma C, Pittenger MF, Cahill KS, Byrne BJ, Kessler PD “Human mesenchymal stem cells differentiate to a cardiomyocyte phenotype in the adult murine heart”. Circulation 105:93-98
- Wakitani S, Saito T, Caplan AI (1995) “Myogenic cells derived from rat bone marrow mesenchymal stem cells exposed to 5-azacytidine”. Muscle Nerve 18:1417-1426
- Munoz-Elias G, Woodbury D, Black IB (2003) “Marrow stromal cells, mitosis, and neuronal differentiation: stem cell and precursor functions”. Stem Cells 21:437-448
- Ferrari G, Cusella-De Angelis G, Coletta M, Paolucci E, Stornaiuolo A, Cossu G, Mavilio F “Muscle regeneration by bone marrow-derived myogenic progenitors”. Science 279:1528-1530
- Devine MJ, Mierisch CM, Jang E, Anderson PC, Balian G (2002) “Transplanted bone marrow cells localize to fracture callus in a mouse model”. J Orthop Res 20:1232-1239
- T L Feldbush 1, D Lafrenz “Alkaline phosphatase on activated B cells characterization of the expression of alkaline phosphatase on activated B cells. Kinetics and membrane anchor” Journal of Immunology. 1991 Dec 1;147(11):3690-5
- Sarah A. Althwaiqeb; Bruno Bordoni “Histology, B Cell Lymphocyte”, StatPearls, May 29, 2023
- Veronica Stahl, Kumar Vasudevan (January 29, 2020) “Comparison of Efficacy of Cannabinoids versus Commercial Oral Care Products in Reducing Bacterial Content from Dental Plaque: A Preliminary Observation”. A Preliminary Observation. Cureus 12(1): e6809
- Schwach-Abdellaoui K, Vivien-Castioni N, Gurny R “Local delivery of antimicrobial agents for the treatment of periodontal diseases”. European Journal of Pharmacology and Biopharmacology 2000, 50:83-99
- “What is Gum (Periodontal) Disease?” The Oral Health Specialists
- Giovanni Appendino et. al. “Antibacterial Cannabinoids from Cannabis satiWa: A Structure-Activity Study” Journal of Natural Products 2008, 71, 1427–1430
- I.G. Karniol, I. Shirakawa, R.N. Takahashi, E. Knobel, R.E. Musty “Effects of delta9-tetrahydrocannabinol and cannabinol in man” Pharmacology, 1975;13(6):502-12
- L E Hollister, H Gillespie “Interactions in man of delta-9-tetrahydrocannabinol. II. Cannabinol and cannabidiol” Clinical Pharmacology Ther. 1975 Jul;18(1):80-3
- Jamie Corroon “Cannabinol and Sleep: Separating Fact from Fiction” Cannabis Cannabinoid Res. 2021 Oct;6(5):366-371
- Isobel Lavender et.al. “Cannabinol (CBN; 30 and 300 mg) effects on sleep and next-day function in insomnia disorder (‘CUPID’ study): protocol for a randomised, double-blind, placebo-controlled, cross-over, three-arm, proof-of-concept trial”. BMJ Open. 2023; 13(8): e071148
- Jason Wallach “Medicinal Cannabis: an overview for health-care providers” 5.13 Cannabinol, Remington (Twenty-third Edition), 2021
- Ethan B. Russo, Jahan Marcu “Cannabinoid Pharmacology”, Advances in Pharmacology, 2017
- Arno Hazekamp et al., wt Development & Modification of Bioactivity, Comprehensive Natural Products II, 2010

Reviewed By:
Vardan Ter-Antonyan
Manager, R&D Formulations
Research & Development