Most of the conversation around the Substance Access Beneficiary Engagement Incentive (BEI) — and healthcare-aligned cannabinoid programs more broadly — is rightly focused on regulation, compliance, and program design. Those are the headline issues.
But sitting underneath them is a quieter, more technical question that brands preparing for this market should be thinking about: how does the ingredient actually get into the body, and how predictably? That’s a delivery technology problem and it’s one of the strongest reasons water-soluble ingredients are positioned to play an outsized role in the next phase of the industry.
First, a quick primer: what is bioavailability?
Bioavailability is the percentage of a substance that reaches the bloodstream and is available for the body to use. It is not what’s on the label. It is what the body absorbs.
The math is straightforward:
Bioavailability (%) = (amount absorbed into the bloodstream) ÷ (amount taken) × 100%
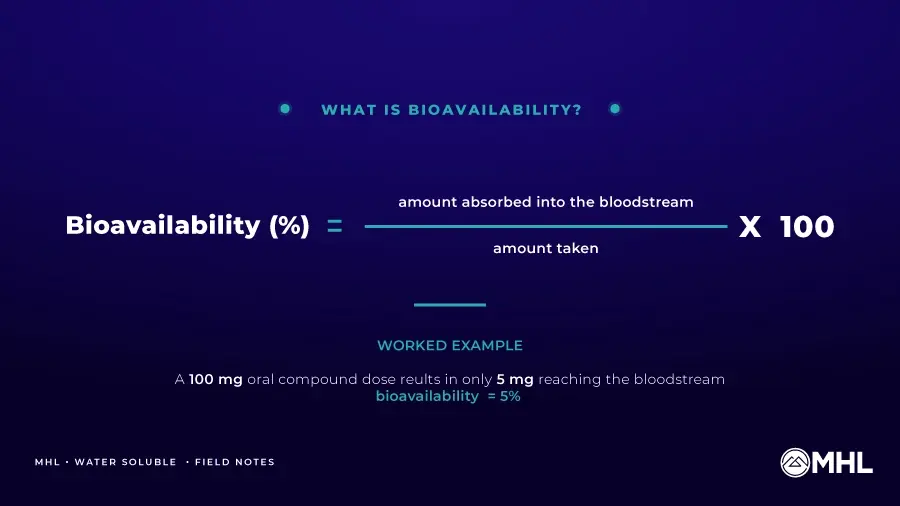
If a patient takes a 100mg oral dose and only 5mg reaches systemic circulation, the bioavailability of that product is 5%. The other 95mg is never absorbed. That gap — between what is labeled and what is biologically usable — is the central technical problem lipophilic oral ingredients have always had.
For wellness products sold at retail, the gap has been tolerable. The consumer takes their tincture, feels something or doesn’t, and adjusts. Outcome data isn’t part of the equation. For programs operating in clinician guided care environments, it is.
The barriers to absorption
Several physiological barriers reduce how much of an orally administered compound actually reaches the bloodstream:
- Poor water solubility. The human body is mostly water. Compounds that don’t dissolve in water — those that are highly lipophilic have a hard time being absorbed in the gastrointestinal tract.
- Stomach acid and digestive enzymes. Digestive processes break down many compounds before they have a chance to be absorbed.
- The gut wall. Only molecules of the right size, shape, and chemistry pass efficiently through intestinal tissue into the bloodstream.
- First-pass metabolism. Once absorbed, compounds travel to the liver, where enzymes break down a significant portion before they can reach systemic circulation.
- Distribution losses. Even after surviving the liver, only a fraction of the original dose typically reaches the target tissues where it can produce a measurable effect.
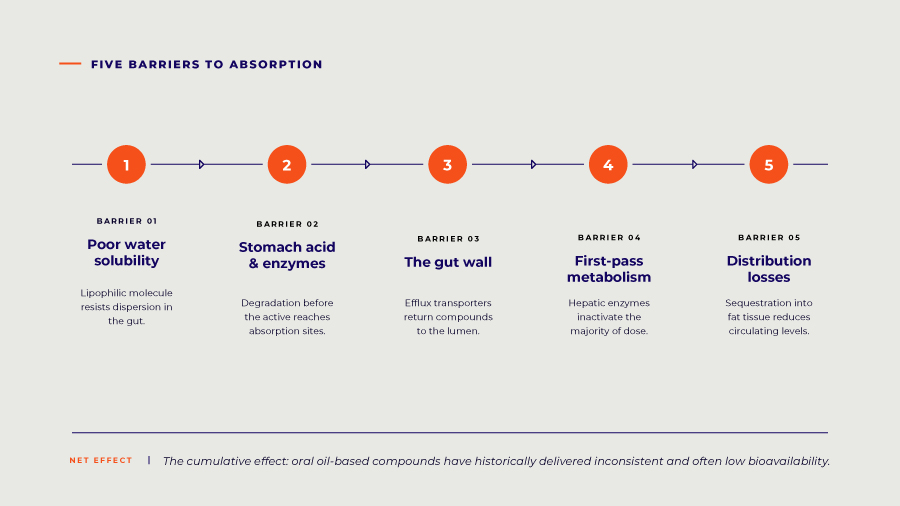
The cumulative effect of these barriers is why oil-based formulations have historically delivered inconsistent and often low bioavailability, with substantial variability from one dose to the next — even within the same person. The challenge isn’t unique to any one compound; many orally administered compounds face the same gauntlet. But lipophilic compounds are particularly affected because of their lipophilic chemistry.
Why this matters more for healthcare-aligned applications
Programs like BEI exist to evaluate outcome-based data under physician supervision. Across the patient support areas defined withing the program framework, the entire premise depends on a chain of inference: the patient took the product, the ingredient achieved consistent absorption, and the program can evaluate outcomes.
If the first link in that chain — absorption — varies meaningfully between doses or between patients, the outcome data downstream becomes much harder to interpret. A clinician can’t reliably distinguish “the dose was inadequate” from “the dose didn’t reach systemic circulation.” An ACO can’t build evidence around products whose absorption profiles change from one dose to the next. A brand can’t defend claims about what their product accomplishes if the upstream variable is unpredictable.
Predictable bioavailability isn’t a marketing nicety in this context. It’s a precondition for the outcome tracking healthcare-aligned programs are built on.
The technologies designed to address it
The pharmaceutical and ingredient industries have developed a range of delivery technologies aimed at improving bioavailability for compounds that struggle with the barriers above. Peer-reviewed work in pharmaceutical journals has examined nano emulsions, lipid-based nanocarriers, self-emulsifying drug delivery systems, and related technologies aimed at the same fundamental goal – improving absorption past the limitations of cannabinoids’ native chemistry.
The most established categories include:
- Micelles — microscopic droplets in which fat-soluble compounds are surrounded by amphiphilic molecules, allowing them to disperse in water-based systems
- Liposomes — spherical, membrane-like structures that encapsulate compounds and offer some protection from degradation in the digestive tract
- Nano- and microemulsions — extremely small, stable droplets with high surface-area-to-volume rations that improve dispersion in water-based systems.
- Self-emulsifying drug delivery systems (SNEDDS / SMEDDS)— formulations that spontaneously form fine droplets when they encounter aqueous environments in the body, improving dissolution and absorption
- Cyclodextrin inclusion complexes — molecular structures that “cage” hydrophobic compounds in water-friendly carriers, supporting their dispersion
Each approach has tradeoffs in stability, manufacturability, cost, and how cleanly it translates to consumer-product formats. The general direction, though, is consistent across the literature: smaller particles, better dispersion in water, and improved formulation performance. Microemulsion-based water-soluble ingredients are one of the most commercially mature applications of this thinking — the compound is broken into nano-scale droplets and stabilized within a water-compatible system, producing a formulation that disperses uniformly into liquid systems and supports dose-to-dose formulation performance compared to tradition oil-based equivalents.
For product format, the implications are direct: water-soluble cannabinoids enable beverages, dissolvable powders, controlled-dose gummies, and other oral formats that simply don’t work with oil-based ingredients. For physicians and program designers, the implications matter more: the dose can be trusted to behave the same way, and that consistency is what makes outcome tracking meaningful: the dose can be trusted to behave the same way, and that consistency is what makes outcome tracking meaningful.
Where MHL’s water-soluble technology fits
MHL’s water-soluble cannabinoid formulations use advanced microemulsion technology and integrate seamlessly into liquid systems. A few specifications are worth understanding:
- Up to 20% loading (200,000 mg/L)— the highest concentration commercially available in the industry, giving formulators significantly more flexibility on final-product design
- Customizable particle size capabilities — important for tuning a formulation to a specific delivery format
- Designed for scalable, repeatable formulations— consistent batch-to-batch performance, which is what GMP-aligned manufacturing requires
Underneath those specifications is the broader regulatory and quality stack that gives water-soluble claims credibility in a healthcare context: completed toxicology studies, NSF GMP-compliant infrastructure, and third-party testing on every lot. Bioavailability claims become much more credible when the ingredient sitting behind them has cleared the regulatory hurdles healthcare-oriented programs are converging on.
Mapping water-soluble to BEI requirements
It’s worth being explicit about how the technology maps to specific BEI eligibility criteria:
- Oral formats only (inhalables excluded): Water-soluble is purpose-built for the oral delivery formats BEI permits — beverages, gummies, dissolvable powders, tinctures.
- ≤ 3mg THC per serving: Water-soluble formulations enable precise, controlled-dose engineering at the serving level, supporting compliance with strict per-serving limits.
- GMP-compliant manufacturing: MHL’s water-soluble production runs through the same NSF GMP infrastructure as the rest of its ingredient portfolio.
Each of these is a place where water-soluble technology turns a BEI requirement from a check-the-box item into a real product advantage.
What brands should be asking now
If your brand is building toward the Substance Access Beneficiary Engagement Incentive (BEI) specifically or the broader category it points toward — a few questions are worth working through:
- Can your current ingredient supply chain deliver consistent bioavailability across batches and across patients?
- How are you positioned to support oral-only product formats at the dose precision physician-supervised programs require?
- Is your current bioavailability story defensible if a clinician or program operator asks for the underlying data?
- Are you exploring water-soluble integration now, while the market is still forming, or planning to retrofit when standards harden?
The brands that take these questions seriously now will have a meaningfully easier path as those programs scale.
In Summary
BEI itself remains pilot-stage and limited in scope. But the technical bar it implies — predictable absorption, controlled dosing, oral-format compatibility, manufacturing consistency — is the bar programs are converging on more broadly.
If you’re evaluating where water-soluble fits in your roadmap, Mile High Labs is ready to support that conversation.
Disclaimer: This article describes a federal pilot program and the technical considerations relevant to ingredient suppliers operating in the hemp-derived CBD category. Nothing herein constitutes a claim regarding the therapeutic value of any product. For official program details, consult the CMS Substance Access Beneficiary Engagement Incentive page.